- Introduction
- How frequent is tinnitus?
- There are many forms of tinnitus
- Animal models of tinnitus
- What is different in the brain of tinnitus patients?
- How is tinnitus generated?
- Clinical trial methodology
- What is important in the diagnosis of tinnitus?
- How efficient are the established therapies?
- Which promising new treatment options are under development?
- What can currently be recommended for the management of tinnitus?
- Concluding Remark
- References
For decades the mechanisms underlying tinnitus have been unknown. It has been assumed that tinnitus is generated in the inner ear. However no “tinnitus generator” could be localized in the inner ear. Moreover all treatment concepts that aimed to induce therapeutic changes in the inner ear failed to improve tinnitus.
In desperate cases the auditory nerve of tinnitus patients was transsected, however this did not result in a reduction of tinnitus – what would be expected if the tinnitus were generated in the inner ear – but rather increased the tinnitus. Animal models and the first neuroimaging studies of tinnitus patients in the nineties demonstrated alterations in the central nervous system. These findings initiated a paradigm shift in tinnitus research in the sense that research was not any more restricted to the ear but also included the central nervous system. Thus tinnitus research became a neuroscientific discipline. This paradigm change resulted in substantial advances in the understanding of the mechanisms involved in the generation of tinnitus and its related symptoms. This deeper understanding resulted in an increasing amount of new ideas about potential treatment strategies, which are currently under development.
This is evidenced by the fact that an increasing amount of tinnitus studies are published in the most prestigious neuroscience journals, but also by the impressive amount of high quality research presented at this year’s TRI meeting which was held under the motto “The neuroscience of tinnitus” and which had more interested attendees than could be accommodated at the conference site. More information about this meeting and the abstract book can be found at www.tinnitusresearch.org.
This article aims to give an overview about the most recent advances in the understanding of the mechanisms involved in the generation of tinnitus and its comorbidies, but also about recent advances in the diagnosis and treatment of tinnitus.
back to top
It has always been known that Tinnitus is a frequent disorder. However data from epidemiologic studies were somewhat contradictory. Two large population based studies demonstrated that tinnitus occurs very frequently in the population.
25.3% of American adults have some form of tinnitus and 7.9% of the population experience it frequently (Shargorodsky, Curhan & Farwell 2010). In a large Norwegian survey of more than 50,000 adults, 21.3% of men and 16.2% of women reported being bothered by their tinnitus, with 4.4% and 2.1%, respectively, reporting high tinnitus intensity (Krog, Engdahl, & Tambs 2010).
These studies are important since they demonstrate that tinnitus is a very frequent problem. These numbers may be helpful to convince both health authorities to perceive tinnitus as a health problem of high socioeconomic relevance and the health industry to invest in tinnitus research.
Moreover tinnitus became a major political issue in the United States since Tinnitus and Hearing Loss are the most frequent health complaint of soldiers returning from Afghanistan and Irak resulting in yearly compensation payments for tinnitus and hearing loss of over 2 billion US $ per year (Yankaskas 2011). Also here there is an increasing motivation in funding tinnitus research for developing more satisfying treatment options in the future.
back to top
There are many forms of tinnitus
Tinnitus is classified according to whether the perceived noise has its source within the patient’s body known as objective tinnitus or somatosounds (for example, myoclonic contractions of the tensor tympani muscle or blood vessels) or if it is only perceivable to the patient and lacks a specific sound source, namely subjective tinnitus. Objective tinnitus is very rare, but in some of the rare cases of objective tinnitus causal treatment is possible. Therefore it is important that the cases of objective tinnitus are not overlooked.
But also subjective tinnitus can have many different forms. Tinnitus can take the form of continuous buzzing, hissing or ringing, or a combination of these or other characteristics. It can be heard in one or both ears, but it can also be refered to the head. Tinnitus can occur intermittently or have a pulsatile character. The intensity of the phantom sound can vary from a subtle noise just above hearing threshold, to high intensity sounds which cannot be masked by any external noise.
Also attention to tinnitus and the accompanying symptoms of tinnitus can vary. The acoustic aspect involves the phantom sound the unwanted sound; ie, most commonly known as the perception of ‘ringing in the ears’. The attentional aspect reflects the extent to which the person is aware of the sound. In addition there are emotional, cognitive and memory components of tinnitus that vary from patient to patient. Many patients with tinnitus report symptoms such as frustration, annoyance, anxiety, depression, irritation and concentration difficulties and these symptoms are highly relevant for the perceived tinnitus severity.
The fact that tinnitus can have many aspects means also that the different forms have different underlying mechanisms and require different treatments. This has consequences for the performance of clinical trials. In order to deal with this situation it has been proposed to assess all potentially relevant clinical characteristics of tinnitus patients in clinical treatment trials and collect the data in large databases. With these data it may be possible in the future to identify characteristics that predict successful treatment outcome for specific therapies (Landgrebe et al. 2010).
back to top
Why are animal models of tinnitus important?
Animal models of tinnitus provide the possibility to exactly identify the neuronal mechanisms of tinnitus generation and to test the effects of various treatments.
But how can tinnitus be induced in animals?
There are different possibilities how tinnitus can be induced in animals. The methods that mimics best the situation in most tinnitus patients is the induction of tinnitus by noise trauma. And how do we know whether an animal perceives tinnitus or not? Also here different methods have been developed. All methods have in common that it is assumed, that animals with tinnitus do not perceive quiet periods any more. By training animals to perform a specific behaviour (e.g. drinking) during quiet times, one can assess, whether animals perceive tinnitus or not. In recent years a sophisticated method has been developed, that requires no training (Turner 2007): A gap in an environmental sound signals a coming loud sound. If this “warning” gap is detected by the animal, its startle reaction to the loud sound is reduced, if not it is not reduced. This method has been shown in many studies to assess whether an animal perceives a phantom sound or not.
Do we know whether animals also suffer from their tinnitus?
This question is more difficult to answer. There are very recent studies, which found behavioural changes in tinnitus animals that resemble those found in animal models of anxiety and depression (Zheng et al. 2011b;Zheng et al. 2011a). But more work will be needed to find out whether these changes recapitulate at least to some extent the suffering of tinnitus patients.
How can animal models help to find new treatments?
For example in animals it is possible to record electrical activity of different areas of the brain by inserted electrodes. This helps to identify the mechanisms involved in tinnitus generation. Even more important the effect of therapeutic interventions on bain activity can be tested. Very recent studies have demonstrates that tinnitus related changes of neuronal activity can be normalized by electrical brain stimulation (Zhang, Zhang, & Zhang 2010), specific drugs (Yang et al. 2011) or a combination of auditory stimulation and vagal nerve stimulation (Engineer et al. 2011). Noteably these findings cannot yet predict whether these treatments will also work in patients with tinnitus. But these findings proof that the proposed treatments are in principle capable to cure tinnitus and they provide first a very promising basis for clinical studies, and second information about important details of the specific treatements. Thus in summary advances in animal models in the last years have provided important contributons to a better understanding of tinnitus and are have recently become an important method in the development of new treatments.
back to top
What is different in the brain of tinnitus patients
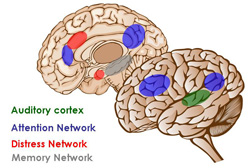
Figure 1: Brain areas involved in tinnitus
EEG and MEG have revealed consistent results across many studies in the sense that in tinnitus the normal activity pattern in the auditory cortex is changed. In the auditory cortex of tinnitus patients alpha activity is reduced, whereas delta and gamma activity is increased. Successful treatment reverses these abnormalities, indicating that they represent the neuronal correlate of tinnitus loudness.
Is neuroimaging useful for clinical diagnosis?
Even if neuroimaging studies have contributed largely to the understanding of tinnitus and have recently been shown to be useful for measuring changes in brain activity induced by successful treatment (Tass et al. 2011), neuroimaging has not yet been developped to a level that it would be useful in clinical diagnostics. Specific patterns of brain activity have been identified as predictors for sprecific treatments (Vanneste et al. 2011), but more studies with large sample sizes will be needed in the future to find out, whether neuroimaging methods will have the potential to predict the success of different treatment interventions.
back to top
In most cases tinnitus is related to hearing problems. However it is not the hearing problems itself that cause tinnitus. Tinnitus is rather the result of the reaction of the brain on impaired hearing.
Most hearing problems are related to the inner ear and within the inner ear to the hair cells that are responsible for the transmission of high frequencies. For example in noise induced hearing loss or age related hearing loss there is preferentially damage of the high frequency regions. As a consequence less information of the high frequency part of sound is transmitted to the brain. The brain in turn tries to compensate for this reduced input and increases the gain of the internal amplifiers. This mechanism is called “homeostatic plasticity”. It has been a debate for many years, whether tinnitus results from the amplification of contrasts between neighboured frequencies with differences in the input. Findings from animal models of tinnitus clearly suggest that it is the homeostatic mechanisms, which are responsible for tinnitus generation. This is an important step forward in the understanding of tinnitus especially since a recent study identified the molecular mechanisms that are involved. This putative mechanism of tinnitus generation also fits with the clinical observation that in most cases the tinnitus frequency is in the same frequency area like the hearing loss. For example a patient with noise trauma induced hearing loss around 4 kHz also perceives the tinnitus at 4 kHz. However tinnitus is not a disease of the auditory system alone. It has already been postulated by Jastreboff more than 20 years ago (Jastreboff 1990), that the difficulty to ignore tinnitus, the annoyance of tinnitus, the anxiety that tinnitus becomes worse, the irritability and the concentration difficulties are related to functional changes in non-auditory brain systems. Neuroimaging studies in tinnitus patients have helped to identify the involved networks in detail (De Ridder et al. 2011a). Thus altered activity in the central auditory pathways is not sufficient for tinnitus perception. This explains that many patients with hearing loss (and consequent increased activity in the central auditory pathways) do not perceive tinnitus. Only when the auditory activity is connected to activity in the “attentional network” the tinnitus is consciously perceived (De Ridder et al. 2011a). If this activity is further accompanied by activation in a “distress network” the patient perceives tinnitus distress. Imaging studies have also demonstrated that the hippocampal area, which plays an important role for memory, is involved in chronic tinnitus. This finding indicates that there may be a “tinnitus memory”, which perpetuates tinnitus perception.
Whether the tinnitus signal is perceived as important and whether the attention focus is kept on the tinnitus, depends on activation of the salience network (De Ridder et al. 2011a). A high salience of the tinnitus signal in turn may increase the perceived loudness of tinnitus by causing increased amplification of the signal in auditory pathways (Rauschecker, Leaver, & Muhlau 2010). This principally useful mechanism of the brain to amplify important information results in case of tinnitus in a vicious circle that contributes to the perpetuation of tinnitus.
Noteably it is important that the different brain networks involved in tinnitus may differ from patient to patient, depending on the specific clinical characteristics. Thus for example in people that are distressed by their tinnitus, the brain activity that is relevant for tinnitus perception is connected to increased activity in the distress network. Moreover earlier findings that the brain activation patterns changes with increasing tinnitus duration have been confirmed (Schecklmann et al. 2011;Vanneste, Van de Heyning, & De Ridder 2011b). This indicates the importance to differentiate between different forms of tinnitus.
back to top
Why is clinical trial methodology important for tinnitus patients?
Only clinical trials will help to find out the efficacy of treatment options. In the past many treatments have been used without any proof of efficacy. Thus patients underwent treatments, even if no clear data were available that provided information about the efficacy of these treatments.
The performance of clinical trials in tinnitus is not trivial for many reasons. First tinnitus is a purely subjective condition, which is difficult to measure. Moreover tinnitus has many aspects, which may be of different relevance in different patients. One patient may be bothered by the loudness of the tinnitus, other patients by the annoyance or the insomnia the tinnitus causes. Moreover specific treatments may be efficient in some patients but not in others.
In the last years valid assessment instruments have been developed for assessing the different aspects of tinnitus. Morfeover it has been systematically investigated which changes in these questionnaire scores are clinically relevant (Zeman et al. 2011). Standardized assessment of clinical characteristics together with systematical collection of these data in large databases (Landgrebe et al. 2010;Witsell et al. 2011) will enable differentiation in clinically relevant subforms of tinnitus.
These developments are essential to bring clinical tinnitus research on a methodologic level that will provide information which treatments are efficient on which aspects of tinnitus in which tinnitus subgroup. This information is essential for further development of evidence based algorithms for the management of tinnitus (Hoare & Hall 2011;Langguth, Kleinjung, & Landgrebe 2011;Searchfield 2011). Moreover the development of methodological standard for clinical tinnitus trials will help to overcome a current barrier which hampers the investment of pharmaceutical companies in the tinnitus field: an internationally accepted standard for clinical trials will provide an orientation what will be required for the approval of newly developed tinnitus drugs.
back to top
What is important in the diagnosis of tinnitus?
As mentioned before there are several forms of tinnitus which differ in the involved neuronal mechanisms. Therefore differential diagnosis is highly important for tinnitus management. First it is important that objective tinnitus is differentiated from subjective tinnitus. A typical form of objective tinnitus is heart synchroneous pulsatile tinnitus, which is frequently due to vascular pathologies such as arterial aneurysma, arteriovenous malformation, stenosis, dissections or due to increased blood flow (e.g. in anemia). These internal sound source can sometimes also be perceived by others (e.g. by auscultation). Thus in all forms of pulsatile tinnitus potential diagnostic testes should be performed to identify vascular abnormalities.
Also in subjective tinnitus the etiology of tinnitus and comorbidities play an important role. Therefore the diagnosis should focus on the etiology of tinnitus and on its comorbidity. In most cases hearing problems are involved in the etiology, but in many cases temporomandibular disorders or neck problems may cause tinnitus as well. In these cases the abnormal somatosensory neuronal input leads to abnormalities in the central auditory pathways which are then perceived as tinnitus. Finally it should be considered that in many cases tinnitus generation is multifactorial. Thus, any combination of altered auditory and somatosensory input together with abnormal activity in central nervous structures (e.g.due to traumatic or ischemic damage or emotional factors) can be relevant for tinnitus generation. Thus, tinnitus which normally disappears spontaneously might persist in the presence of associated stress (De Ridder et al. 2011a). Such a multifactorial genesis may be frequently the case in post-traumatic tinnitus e.g. in blast related tinnitus (Hoffer et al. 2010). Moreover, the factors involved in tinnitus generation may be different from the factors related to the persistence of tinnitus, as illustrated by the fact that many people perceive transient tinnitus after noise trauma but only in a few of them tinnitus becomes permanent (Ortmann et al. 2011).
Thus, various etiologic factors and comorbidities are known to play a role in tinnitus and most likely lead to specific pathophysiologic patterns of neuronal activity. An exact diagnosis is required for the best possible therapeutic management.
back to top
How efficient are the established therapies?
In recent studies the efficacy of many widely used therapies has been analysed. For some treatment forms also meta-amalyses have been performed. In these meta-analyses the results of available controlled studies are pooled ans reanalysed. Positive findings from meta-analyses are generally considered as the highest evidence for efficacy. For cognitive behavioural therapies two meta-analyses demonstrated beneficial effects on quality of life measures, but not on tinnitus loudness (Hesser et al. 2010;Martinez-Devesa et al. 2010). An analysis of different forms of sound therapies came to the conclusion that the available studies are not sufficient to judge the efficacy of this treatment form (Hoare et al. 2011;Hobson, Chisholm, & El Refaie 2010). Interestingly the effects of hearing aids, which are widely used in the management of tinnitus have only been very poorly investigated in the past. A recent study found that only those patients benefit from hearing aids, who perceive their tinnitus below 6 kHz, which is the frequency range, in which hearing aids amplify the sound. Patients who perceive their tinnitus at higher frequencies, (where the hearing aid is not amplifying any more) do not perceive any tinnitus reduiction after hearing aid use (Schaette et al. 2010).
Currently there is no pharmacological substance approved by the Federal food and drug administration (FDA) or the European Medicines Agency (EMA) for the treatment of tinnitus (Elgoyhen & Langguth 2010). Antidepressants are commonly used in the pharmacological protocols for the management of tinnitus. The results of studies investigating antidepressants suggest that these compounds have no direct effect on the tinnitus, but that tinnitus patients with depression and anxiety may gain some benefit from them (Langguth et al. 2011b;Robinson, Viirre, & Stein 2007). Also medications for the treatment of epilepsy have been studied in tinnitus patients, but controlled studies have not demonstrated additional benefits compared to placebo (Hoekstra et al. 2011).
Thus, even if some drugs have been reported to provide moderate relief of symptoms in a subset of patients, no drug has yet proven sufficient effectiveness in randomized controlled clinical trials in order to be approved specifically for tinnitus.
back to top
Which promising new treatment options are under development?
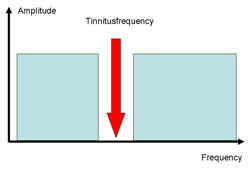
Figure 2: Frequency spectrum of tailor made music
(Okamoto et al. 2010)
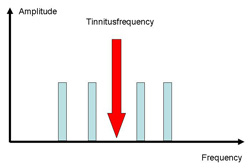
Figure 3: Frequency spectrum of coordinated reset
(Tass et al. 2011)
Very recently, coordinated reset stimulation (Tass & Hauptmann 2007) has been proposed for tinnitus treatment. Based on computational modeling, individualized auditory stimuli above and below the tinnitus frequency are presented as short tones with the aim to renormalize tinnitus related pathologic neuronal synchrony. The publication of the first results from a pilot study is expected (Tass et al. 2011).
Cochlear implants can restore hearing in patients with profound deafness. Frequently profound deafness is accompanied by tinnitus. Whereas the classic indication for cochlear implants has been bilateral hearing loss, new studies demonstrated that unilateral cochlear implants can have very beneficial effects on tinnitus in patients with single-sided profound deafness with concomitant ipsilateral incapacitating tinnitus (Kleinjung et al. 2009;Van de Heyning et al. 2008).
Among new pharmacological approaches the most promising results come from a large study that investigated the substance neramexane, which blocks both glutamatergic NMDA receptors and a9a10 nicotinic cholinergic receptors (Suckfuell et al. 2011). This substance is currently further investigated in several phase III studies.
Various brain stimulation techniques are under investigation. The idea of this approach is to normalize the disturbed neuronal network activity that underlies tinnitus. First attempts stimulated the auditory cortex, either by transcranial magnetic stimulation (Langguth et al. 2008), transcranial direct current stimulation (tDCS) (Garin et al. 2011) or by implanted electrodes (De Ridder et al. 2011b).
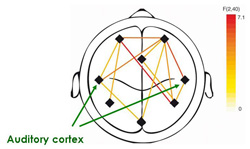
Figure 4: Abnormalities of brain connectivity in
tinnitus (Schlee et al. 2009).
In tinnitus patients the auditiory cortex is more
connected to nonauditory brain areas.

Figure 5: Transcranial magnetic stimulation for the
treatment of tinnitus (Kleinjung & Langguth 2009)
The most studied approach has been rTMS to the temporal cortex, which has shown beneficial effects in several studies (Meng et al. 2011). However the average effect is small and the variability across patients is very high. Therefore further strategies are needed to enhance the effects in order to become relevant for clinical routine (Kleinjung & Langguth 2009).
All techniques presented in this section have been only recently been developed as treatment options for tinnitus. Even if they have shown promising results in pilot studies, none of them have supplied enough evidence for a general application in routine treatment. Being at an early stage of development, an increase in efficacy can be expected for all these methods in the next years, especially with increasing knowledge of both the pathophysiology of the different forms of tinnitus and the neurobiological mechanisms involved in the modulatory effects of the different interventions.
back to top
What can currently be recommended for the management of tinnitus?
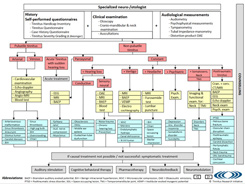
A first effort has been made by a multidisciplinary and multinational team of clinicians (Langguth et al. 2011a) to summarize currently available information in an algorithm for the management of tinnitus patients that is publically available in an interactive form at www.tinnitusresearch.org.
This evidence-based treatment algorithm advocates a structured approach for the diagnosis and treatment of tinnitus, with particular emphasis on awareness of specific subgroups of tinnitus patients who might benefit from tailored treatment (Langguth et al. 2011a). According to this algorithm, all patients initially receive the same diagnostic assessment, the outcomes of which are used to provide a tailored approach to subsequent diagnostic or therapeutic evaluations. This step comprises technical tests that are tailored towards the diagnosis of specific tinnitus-related psychological (for example, depression, anxiety, insomnia) and somatic symptoms. Once diagnosed, causally oriented treatment is recommended, but, for instances in which such treatments are unavailable or unsuccessful, symptomatic treatment options (alongside counseling) should be considered for all patients who are impaired by their tinnitus.
The presented algorithm for the management of tinnitus represents the essential structure of the recently edited Textbook of Tinnitus which provides a multidisciplinary overview of the diagnosis and management of this widespread and troubling disorder. The book emphasizes that tinnitus is not one disease but a group of rather diverse disorders with different pathophysiology, different causes and, consequently, different treatments. The Textbook of Tinnitus describes both the theoretical background of the different forms of tinnitus and it provides detailed knowledge of the state-of-the-art of its treatment. In almost hundred chapters written by experts from many disciplines, the book aims to give an comprehensive overview of the state of the art of tinnitus management.
back to top
Within the last years animal research and neuroimaging have generated a more and more detailed understanding of the pathophysiological mechanisms of the different forms of tinnitus. Alterations in several auditory and nonauditory brain networks have been identified, which reflect the various clinical aspects of tinnitus and which interact dynamically with each other. This knowledge has resulted in new potential therapeutic targets and new treatment approaches, of which many have already shown promising data in „proof of concept“-studies. For most of these new approaches further development is needed before they can be considered established treatments for clinical routine use. Nevertheless the increasing understanding of the pathophysiology and the increasing number of new treatments on the horizon give rise to the hope, that soon better treatment options will become available to help the many tinnitus patients to overcome their daily suffering.
back to top
- De Ridder, D., Elgoyhen, A. B., Romo, R., & Langguth, B. 2011a, "Phantom percepts: Tinnitus and pain as persisting aversive memory networks", Proc.Natl.Acad.Sci.U.S.A, vol. 108, no. 20, pp. 8075-8080.
- De Ridder, D., Vanneste, S., Kovacs, S., Sunaert, S., Menovsky, T., Van de Heyning, P., & Moller, A. 2011b, "Transcranial magnetic stimulation and extradural electrodes implanted on secondary auditory cortex for tinnitus suppression", J Neurosurg.
- Elgoyhen, A. B. & Langguth, B. 2010, "Pharmacological approaches to the treatment of tinnitus", Drug Discov.Today, vol. 15, no. 7-8, pp. 300-305.
- Engineer, N. D., Riley, J. R., Seale, J. D., Vrana, W. A., Shetake, J. A., Sudanagunta, S. P., Borland, M. S., & Kilgard, M. P. 2011, "Reversing pathological neural activity using targeted plasticity", Nature.
- Frank, E., Schecklmann, M., Landgrebe, M., Burger, J., Kreuzer, P., Poeppl, T. B., Kleinjung, T., Hajak, G., & Langguth, B. 2011, "Treatment of chronic tinnitus with repeated sessions of prefrontal transcranial direct current stimulation: outcomes from an open-label pilot study", J Neurol.
- Garin, P., Gilain, C., Van Damme, J. P., de, F. K., Jamart, J., Ossemann, M., & Vandermeeren, Y. 2011, "Short- and long-lasting tinnitus relief induced by transcranial direct current stimulation", J Neurol.
- Hesser, H., Weise, C., Westin, V. Z., & Andersson, G. 2010, "A systematic review and meta-analysis of randomized controlled trials of cognitive-behavioral therapy for tinnitus distress", Clin.Psychol.Rev.
- Hoare, D. J. & Hall, D. A. 2011, "Clinical Guidelines and Practice: A Commentary on the Complexity of Tinnitus Management", Eval.Health Prof.
- Hoare, D. J., Kowalkowski, V. L., Kang, S., & Hall, D. A. 2011, "Systematic review and meta-analyses of randomized controlled trials examining tinnitus management", Laryngoscope, vol. 121, no. 7, pp. 1555-1564.
- Hobson, J., Chisholm, E., & El Refaie, A. 2010, "Sound therapy (masking) in the management of tinnitus in adults", Cochrane Database Syst.Rev. no. 12, p. CD006371.
- Hoekstra, C. E., Rynja, S. P., van Zanten, G. A., & Rovers, M. M. 2011, "Anticonvulsants for tinnitus", Cochrane Database Syst.Rev. no. 7, p. CD007960.
- Hoffer, M. E., Balaban, C., Gottshall, K., Balough, B. J., Maddox, M. R., & Penta, J. R. 2010, "Blast exposure: vestibular consequences and associated characteristics", Otol.Neurotol., vol. 31, no. 2, pp. 232-236.
- Jastreboff, P. J. 1990, "Phantom auditory perception (tinnitus): mechanisms of generation and perception", Neurosci.Res., vol. 8, pp. 221-254.
- Kleinjung, T. & Langguth, B. 2009, "Strategies for enhancement of transcranial magnetic stimulation effects in tinnitus patients", Int.Tinnitus.J, vol. 15, no. 2, pp. 154-160.
- Kleinjung, T., Steffens, T., Strutz, J., & Langguth, B. 2009, "Curing tinnitus with a Cochlear Implant in a patient with unilateral sudden deafness: a case report", Cases.J, vol. 2, p. 7462.
- Krog, N. H., Engdahl, B., & Tambs, K. 2010, "The association between tinnitus and mental health in a general population sample: results from the HUNT Study", J Psychosom.Res., vol. 69, no. 3, pp. 289-298.
- Landgrebe, M., Zeman, F., Koller, M., Eberl, Y., Mohr, M., Reiter, J., Staudinger, S., Hajak, G., & Langguth, B. 2010, "The Tinnitus Research Initiative (TRI) database: a new approach for delineation of tinnitus subtypes and generation of predictors for treatment outcome", BMC.Med.Inform.Decis.Mak., vol. 10, p. 42.
- Langguth, B., Biesinger, E., Del Bo, L., De Ridder, D., Goodey, R., Herraiz, C., Kleinjung, T., Lainez, J. M., Landgrebe, M., Paolino, M., Questier, B., Sanchez, T. G., & Searchfield, G. D. 2011a, "Algorithm for the diagnostic and therapeutic management of tinnitus," in Textbook of Tinnitus, 1 edn, A. Moller et al., eds., Springer, pp. 381-385.
- Langguth, B., De Ridder, D., Dornhoffer, J. L., Eichhammer, P., Folmer, R. L. F. E., Fregni, F., Gerloff, C., Khedr, E., Kleinjung, T., Landgrebe, M., lee, S., Lefaucheur, J. P., Londero, A., Marcondes, R., Moller, A. R., Pascual-Leone, A., Plewnia, C., Rossi, S., Sanchez, T., Sand P.G., Schlee, W., Steffens, T., Van de Heyning, P., & Hajak, G. 2008, "Does rTMS/tDCS show efficacy in treating tinnitus patients?", Brain Stimulation, vol. 1, no. 3, pp. 192-205.
- Langguth, B., Kleinjung, T., & Landgrebe, M. 2011, "Tinnitus: The Complexity of Standardization", Eval.Health Prof.
- Langguth, B., Kleinjung, T., Landgrebe, M., De Ridder, D., & Hajak, G. 2010, "rTMS for the treatment of tinnitus: the role of neuronavigation for coil positioning", Neurophysiol.Clin., vol. 40, no. 1, pp. 45-58.
- Langguth, B., Landgrebe, M., Kleinjung, T., Sand, G. P., & Hajak, G. 2011b, "Tinnitus and depression", World J Biol.Psychiatry.
- Martinez-Devesa, P., Perera, R., Theodoulou, M., & Waddell, A. 2010, "Cognitive behavioural therapy for tinnitus", Cochrane Database Syst.Rev. no. 9, p. CD005233.
- Meng, Z., Liu, S., Zheng, Y., & Phillips, J. S. 2011, "Repetitive transcranial magnetic stimulation for tinnitus", Cochrane Database Syst.Rev., vol. 10, p. CD007946.
- Okamoto, H., Stracke, H., Stoll, W., & Pantev, C. 2010, "Listening to tailor-made notched music reduces tinnitus loudness and tinnitus-related auditory cortex activity", Proc.Natl.Acad.Sci.U.S.A, vol. 107, no. 3, pp. 1207-1210.
- Ortmann, M., Muller, N., Schlee, W., & Weisz, N. 2011, "Rapid increases of gamma power in the auditory cortex following noise trauma in humans", Eur.J Neurosci., vol. 33, no. 3, pp. 568-575.
- Rauschecker, J. P., Leaver, A. M., & Muhlau, M. 2010, "Tuning out the noise: limbic-auditory interactions in tinnitus", Neuron, vol. 66, no. 6, pp. 819-826.
- Robinson, S. K., Viirre, E. S., & Stein, M. B. 2007, "Antidepressant therapy in tinnitus", Hear.Res., vol. 226, no. 1-2, pp. 221-231.
- Schaette, R., Konig, O., Hornig, D., Gross, M., & Kempter, R. 2010, "Acoustic stimulation treatments against tinnitus could be most effective when tinnitus pitch is within the stimulated frequency range", Hear Res., vol. 269, no. 1-2, pp. 95-101.
- Schecklmann, M., Landgrebe, M., Poeppl, T. B., Kreuzer, P., Manner, P., Marienhagen, J., Wack, D. S., Kleinjung, T., Hajak, G., & Langguth, B. 2011, "Neural correlates of tinnitus duration and Distress: A positron emission tomography study", Hum.Brain Mapp.
- Schlee, W., Hartmann, T., Langguth B, & Weisz, N. 2009, "Abnormal resting-state cortical coupling in chronic tinnitus", BMC.Neurosci., vol. 10, no. 11.
- Searchfield, G. 2011, "A Commentary on the Complexity of Tinnitus Management: Clinical Guidelines Provide a Path Through the fog", Eval.Health Prof.
- Shargorodsky, J., Curhan, G. C., & Farwell, W. R. 2010, "Prevalence and characteristics of tinnitus among US adults", Am.J Med., vol. 123, no. 8, pp. 711-718.
- Stracke, H., Okamoto, H., & Pantev, C. 2010, "Customized notched music training reduces tinnitus loudness", Commun.Integr.Biol., vol. 3, no. 3, pp. 274-277.
- Suckfuell, M., Althaus, M., Ellers-Lenz, B., Gebauer, A., Goertelmeyer, R., Jastreboff, P. J., Moebius, H. J., Rosenberg, T., Russ, H., Wirth, Y., & Krueger, H. 2011, "A randomized, double-blind, placebo-controlled clinical trial to evaluate the efficacy and safety of neramexane in patients with moderate to severe subjective tinnitus", BMC.Ear Nose Throat Disord., vol. 11, no. 1, p. 1.
- Tass, P. A. and others. Counteracting Tinnitus Symptoms And Related Pathological Cerebral Synchrony By Acoustic Coordinated Reset Neuromodulation. Abstract Book, 5th International TRI Tinnitus Conference . 2011.
- Tass, P. A. & Hauptmann, C. 2007, "Therapeutic modulation of synaptic connectivity with desynchronizing brain stimulation", Int.J Psychophysiol., vol. 64, no. 1, pp. 53-61.
- Turner, J. G. 2007, "Behavioral measures of tinnitus in laboratory animals", Prog.Brain Res., vol. 166, pp. 147-156.
- Van de Heyning, P., Vermeire, K., Diebl, M., Nopp, P., Anderson, I., & De Ridder, D. 2008, "Incapacitating unilateral tinnitus in single-sided deafness treated by cochlear implantation", Ann.Otol.Rhinol.Laryngol., vol. 117, no. 9, pp. 645-652.
- Vanneste, S. & De Ridder, D. 2011, "Bifrontal transcranial direct current stimulation modulates tinnitus intensity and tinnitus-distress-related brain activity", Eur.J Neurosci., vol. 34, no. 4, pp. 605-614.
- Vanneste, S., Focquaert, F., Van de Heyning, P., & De Ridder, D. 2011, "Different resting state brain activity and functional connectivity in patients who respond and not respond to bifrontal tDCS for tinnitus suppression", Exp.Brain Res., vol. 210, no. 2, pp. 217-227.
- Vanneste, S., Plazier, M., Ost, J., van der Loo, E., Van de Heyning, P., & De Ridder, D. 2010, "Bilateral dorsolateral prefrontal cortex modulation for tinnitus by transcranial direct current stimulation: a preliminary clinical study", Exp.Brain Res., vol. 202, no. 4, pp. 779-785.
- Vanneste, S., Van de Heyning, P., & De Ridder, D. 2011a, "Contralateral parahippocampal gamma-band activity determines noise-like tinnitus laterality: a region of interest analysis", Neuroscience.
- Vanneste, S., Van de Heyning, P., & De Ridder, D. 2011b, "The neural network of phantom sound changes over time: a comparison between recent-onset and chronic tinnitus patients", Eur.J Neurosci., vol. 34, no. 5, pp. 718-731.
- Witsell, D. L., Schulz, K. A., Moore, K., & Tucci, D. L. 2011, "Implementation and testing of research infrastructure for practice-based research in hearing and communication disorders", Otolaryngol.Head Neck Surg., vol. 145, no. 4, pp. 565-571.
- Yang, S., Weiner, B. D., Zhang, L. S., Cho, S. J., & Bao, S. 2011, "Homeostatic plasticity drives tinnitus perception in an animal model", Proc.Natl.Acad.Sci.U.S.A, vol. 108, no. 36, pp. 14974-14979.
- Yankaskas, K. Operational Readiness: The Role of Tinnitus Research. Abstract Book, 5th International TRI Tinnitus Conference . 2011.
- Zeman, F., Koller, M., Figueiredo, R., Aazevedo, A., Rates, M., Coelho, C., Kleinjung, T., De, R. D., Langguth, B., & Landgrebe, M. 2011, "Tinnitus Handicap Inventory for Evaluating Treatment Effects: Which Changes Are Clinically Relevant?", Otolaryngol.Head Neck Surg.
- Zhang, J., Zhang, Y., & Zhang, X. 2010, "Auditory Cortex Electrical Stimulation Suppresses Tinnitus in Rats", J Assoc.Res.Otolaryngol.
- Zheng, Y., Hamilton, E., McNamara, E., Smith, P. F., & Darlington, C. L. 2011a, "The effects of chronic tinnitus caused by acoustic trauma on social behaviour and anxiety in rats", Neuroscience, vol. 193, pp. 143-153.
- Zheng, Y., Hamilton, E., Stiles, L., McNamara, E., de, W. C., Smith, P. F., & Darlington, C. L. 2011b, "Acoustic trauma that can cause tinnitus impairs impulsive control but not performance accuracy in the 5-choice serial reaction time task in rats", Neuroscience, vol. 180, pp. 75-84.
- back to top
Author:
Berthold Langguth, MD, PhD
Interdisciplinary Tinnitus Clinic
Department of Psychiatry and Psychotherapy, University of Regensburg, Germany
Universitaetsstraße 84
93053 Regensburg – Germany
E-mail: